What Is ACL Reconstruction?
ACL reconstruction replaces a torn ligament with a graft harvested from hamstring, quadriceps, or donor tissue. Using arthroscopic guidance and computer-mapped tunnels, the new ligament is positioned exactly where the native ACL once sat, restoring stability for sports that involve cutting, pivoting, or sudden stops.
Graft Options
- Hamstring autograft: Popular for balanced strength and low donor-site pain.
- Quadriceps tendon graft: Thicker graft suited for high-demand athletes or revisions.
- Bone–patellar tendon–bone (BPTB): Excellent fixation for contact athletes or those with hyperlaxity.
- Allograft: Considered for multi-ligament injuries or patients preferring no additional incisions.
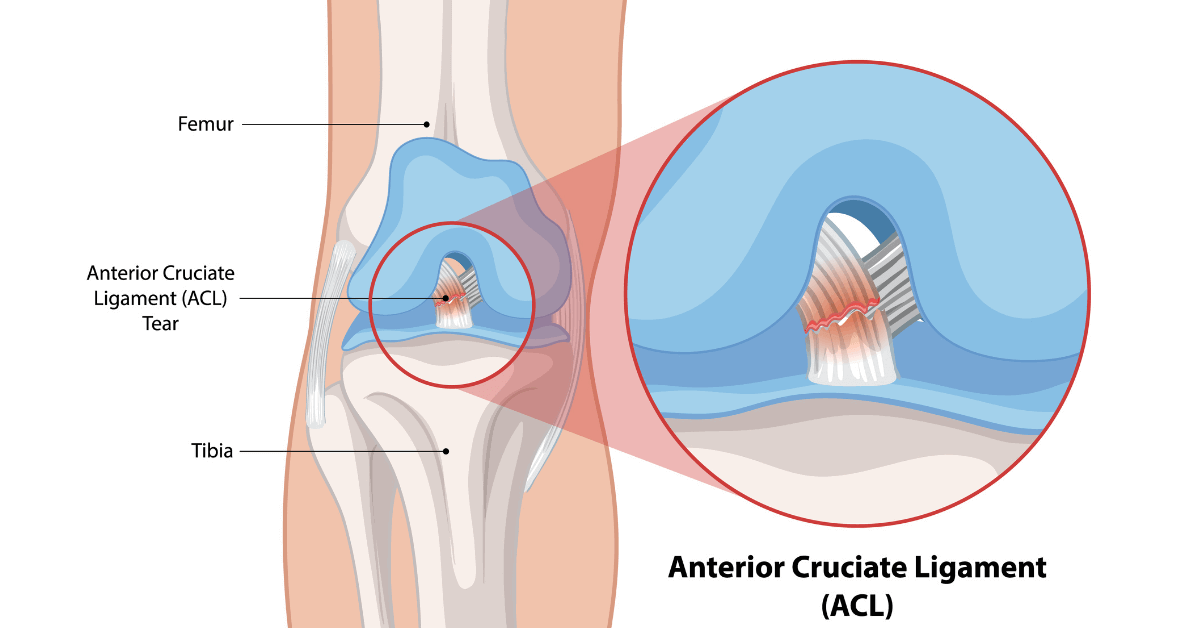
Who Needs ACL Reconstruction?
ACL tears rarely heal on their own. Reconstruction is recommended when instability affects daily life or sports participation.
- Pivoting athletes: Football, basketball, badminton, and kabaddi players with giving-way episodes.
- Combined meniscus injuries: Meniscus repair outcomes improve when the ACL is stabilised.
- Active professionals: Individuals whose jobs demand climbing, jumping, or rapid directional change.
- Chronic instability: Repeated buckling that leads to cartilage damage or early arthritis.
MRI, KT-1000 laxity testing, and gait analysis help quantify instability and plan the reconstruction strategy.
How the Procedure Works
ACL reconstruction is a day-care arthroscopic procedure with minimal incisions and rapid recovery.
- Graft harvest: Selected tendon is prepared with precise diameter and length.
- Arthroscopic assessment: Meniscus tears or cartilage lesions are treated in the same sitting.
- Tunnel drilling: Guides create femoral and tibial tunnels that mirror the original ACL footprints.
- Graft fixation: Suspensory buttons or interference screws secure the graft before cycling the knee to confirm tension.
Benefits of Anatomic ACL Surgery
- Reliable stability: Prevents giving-way episodes during sport or daily movement.
- Meniscus protection: Stable knees reduce the risk of secondary meniscus tears.
- Return to sport: Athletes regain cutting, sprinting, and jumping capacity with structured rehab.
- Arthritis prevention: Early stabilisation reduces abnormal joint loading over time.
Rehabilitation Timeline
- Week 0–2: Swelling control, full extension, and quadriceps activation.
- Week 3–6: Progressive weight-bearing, closed-chain strengthening, and balance drills.
- Month 3: Jogging, plyometrics, and sport-specific agility under supervision.
- Month 6–9: Return-to-play testing including hop tests and strength symmetry checks.
- Ongoing: Neuromuscular training to prevent re-injury and optimise performance.
Risks and Mitigation
ACL reconstruction is remarkably safe, and our protocols further reduce complications.
- Graft failure: Prevented with accurate tunnel placement, proper rehabilitation, and return-to-sport criteria.
- Infection: Rare due to arthroscopic technique and stringent sterilisation.
- Loss of motion: Avoided with early extension exercises and scar management.
- Donor-site discomfort: Addressed through targeted physiotherapy and gradual loading.
- Blood clots: Minimised with early mobilisation and hydration.
Our sports medicine team guides athletes through mental readiness, nutrition, and injury-prevention strategies for long-term success.